
Do Cold Sores Cause Alzheimer's?
What's the connection, and what should you do about it?

Sarah from Ireland asks:
“How big a risk factor are cold sores / HSV-1 for Alzheimer’s? I am concerned as I get them a lot and I also have one copy of ApoE4?”
It’s a great question, as a growing body of evidence points towards a connection between HSV1 infections and Alzheimer’s Disease (AD).
So, in this post, we’ll review the key evidence, what to make of it, and what to do about it if you get cold sores.
As you’ll see, the discussion gets to some critical issues around how we think about AD in the first place. Click below to listen to the Better Brain Fitness episode where we answer this question, or read on.
Background: Herpes Simplex Viruses and The Brain
Cold sores, those painful blisters that erupt around your mouth when you’re getting ready for prom or a major television appearance, are caused by the Herpes Simplex Virus Type 1 (HSV1). It is one of eight herpes viruses that can infect humans. The formal term for it is “herpes labialis” (herpes of the lips).
All herpes viruses exhibit a similar behavior pattern: after causing an initial infection, they go into hiding somewhere in the body. That means that once we’ve got them, we’ve got them for good.
Importantly for our discussion, certain strains of the herpes virus like to hide out in nerve tissue.
For instance, the initial infection of HSV1 typically causes blisters in the mouth and around the face, sometimes accompanied by other symptoms of systemic infection like fever and malaise. After that initial infection clears, the virus travels up the sensory nerves of the face to their hideout in the trigeminal ganglia of the brainstem (where the cell bodies for those nerves are located), where they remain indefinitely.
If the virus awakens from its slumber, or “reactivates,” it can travel up those facial nerves towards the skin, causing another round of blisters, which we know as cold sores (or “fever blisters”).
In some cases, the reactivated virus can take a different route, traveling instead from its home in the trigeminal ganglion along nerves to the temporal lobe, producing a much more severe and sometimes lethal infection of brain tissue known as HSV Encephalitis (or just “Herpes Encephalitis”). This produces a clinical syndrome that in some ways looks like a very rapid progressive Alzheimer’s disease, as it involves similar parts of the brain.
Another familiar member of the herpes virus with an affinity for nerve tissue is Varicella Zoster, or VZV. The initial infection of VZV causes the syndrome we know as “chicken pox” (one of several miserable childhood rites of passage ended by vaccines). Once chicken pox clears, VZV hides out in the dorsal root ganglion of the spinal cord, where the cell bodies for the nerves that supply the skin of our torso are located. If reactivated, it can travel down one of those nerves, causing blisters on the torso that we know as shingles.
So, the key takeaway here is that, once we’re infected with it once, the virus that causes cold sores (HSV1) lives inside of us indefinitely, and shows a special attraction to areas of the brain known to be impacted early in Alzheimer’s.
Given that behavior, it’s not too much of a stretch to wonder whether HSV contributes in some way to Alzheimer’s.
Table. Herpes viruses that hide in nerves.

The HSV-AD Connection: What’s the evidence?
So, the fact HSV1 likes to live inside and infect brain tissue certainly makes a connection to AD plausible. But what actual evidence supports such a connection?
EXHIBIT A: HSV DNA is commonly found in the brains of those with Alzheimer’s.
In the 1980s, published studies showed HSV DNA in the brains of individuals with Alzheimer's. Furthermore, the DNA was often found in amyloid plaques which, at the time, were considered the defining brain pathology of AD. This observation made the HSV-AD connection seem even more plausible, though the theory didn’t get much traction then.
But, recent research has provided more evidence supporting a connection, reigniting interest in this hypothesis.
First, more studies have confirmed that the brains of those with AD are more likely to have HSV DNA in them than controls, and that the DNA is commonly found in amyloid plaques (in one autopsy study, HSV DNA was found in 90 percent of amyloid plaques).
EXHIBIT B: Evidence of prior HSV infection is associated with a heightened risk of Alzheimer’s.
Other studies have shown that the presence of HSV antibodies in the blood, indicating exposure to the virus, increases the likelihood of developing AD. In one study of 270 people with AD and 270 controls, those with AD were 2.25 times more likely to have HSV antibodies in their blood than those without it.
A study from South Korea using their national health insurance service database followed patients over the age of 50 for eight years. Over that time, about 90,000 people had a symptomatic HSV infection and around 90,000 had a symptomatic VZV infection. Those two groups were then compared to a control group of 180,000.
During this eight year follow up, a little over 17% of the people who’d had HSV infections went on to be diagnosed with Alzheimer's, about 17.5% with VZV infections were diagnosed with it, compared to 14% of those in the control group. Based on that data, those with herpes virus antibodies were 1.18 times more likely to be diagnosed with AD.
EXHIBIT C: The ApoE4 genotype is associated with an increase in HSV recurrence.
Interestingly, the ApoE4 genotype, known to increase AD risk, also heightens the likelihood of HSV1 recurrence. This suggests the possibility that ApoE4 elevates AD risk by increasing susceptibility to HSV infections.
But…not all data points to a connection.
In an analysis done as part of the Rotterdam study in the Netherlands, HSV antibodies were associated with “subtle cognitive disturbances” but not a heightened risk of AD.
Additionally, not all Alzheimer's brains have HSV DNA, not all with HSV antibodies in their blood develop AD, not all with AD have HSV antibodies, and not all with HSV DNA detected in brain autopsies have AD.
Resolving The Contradiction
Based on the data we have, you might be inclined to think that the evidence around HSV and AD is contradictory and thus inconclusive.
This would be true if Alzheimer’s had a single cause, or a “smoking gun”.
We’ve certainly been conditioned to think this way about the disease. The majority of Alzheimer’s research has been based on the assumption of a single cause. It’s a seductive idea, because single causes can have single “cures”.
For years now, the prime-smoking-gun-suspect has been beta-amyloid plaque. All of the major drug trials that have been conducted in recent years have been for medications that target beta-amyloid. You probably know how that has turned out.

To be fair, other factors can contribute to disease risk under the amyloid-smoking-gun model. But, in that model, all roads must still somehow lead to amyloid (including HSV1 infection).

While it continues to have its proponents, there are all sorts of problem with the amyloid model (well beyond the scope of this discussion, but discussed in part here). In our view, linking the involvment of HSV to AD to its connection to amyloid undermines more than it strengthens the argument. Amyloid may even be playing a beneficial role by limiting the virus’s spread, rather than contributing to disease pathology.
But the even bigger problem is the assumption that there’s a smoking gun to begin with.
It just isn’t possible to reconcile all that we now know about AD with the idea of a single cause. This shouldn’t be surprising, as almost all biological phenomena are much more complex than that (and the story behind why we were drawn to that improbable assumption in the first place is one for a future post). But the smoking-gun assumption is largely responsible for decades of disappointment in AD treatment research (as is true for most common afflictions of our day).
At this point, it is clear that AD results from the combined effect of many different factors. Furthermore, the impact of those factors is contextual, meaning that the particular contribution of any one factor is entirely contingent upon what other factors are present. Their effects cannot be understood in isolation.

As mentioned, reconciling all of the existing HSV data with a single-cause model is impossible.
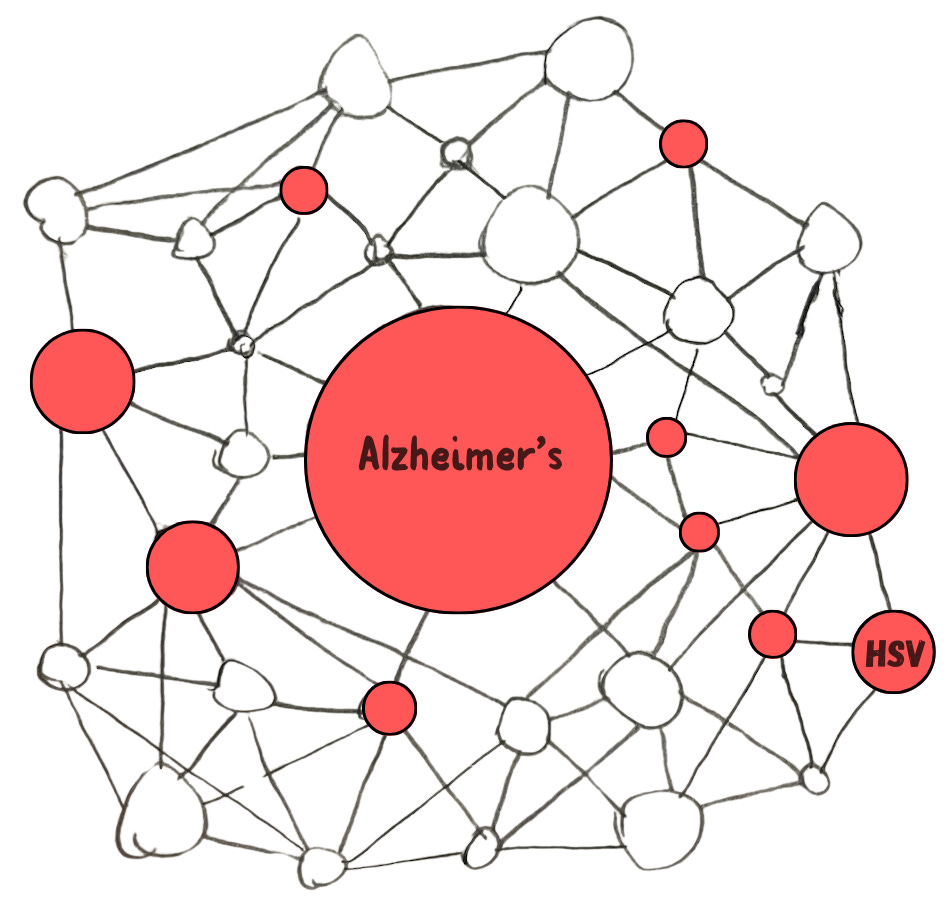
However, reconciling the HSV data (along with all of the other risk factor data) with a systems-based, multifactorial model is entirely possible. In some cases of AD, HSV reactivations are a contributing factor:
In other cases of AD, they are not.
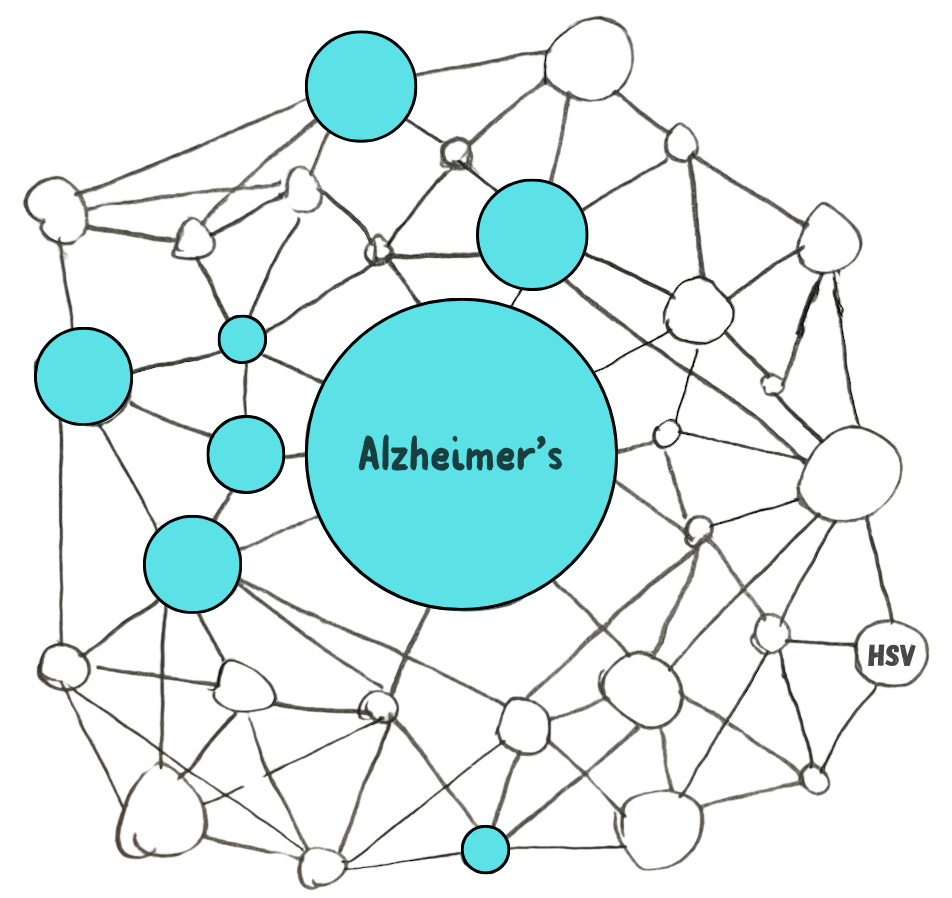
For some people, recurrent HSV infections increase their risk of AD. For others, it does not. Again, the impact is contextual.

It’s complex and messy. Welcome to biology.
Does Treating HSV With Anti-Virals Help Prevent Alzheimer’s?
There are three anti-viral medications - acyclovir, famcyclovir and valacyclovir - which are effective at treating and preventing HSV reactivation infections (they do not eradicate the viruses from their hideouts, however).
So, if HSV reactivation does indeed contribute to the development of AD in some cases, then could taking an antiviral regularly to prevent reactivations reduce the risk of AD in those cases?
It’s an important question, but not one we have a clear answer to yet.
The good news is that there are several trials going on right now, including one that’s testing daily anti-viral therapy (valacyclovir 2-4 grams per day) in those with HSV antibodies, the ApoE4 genotype, and early AD.
What To Do Now?
So back to Sarah’s original question...
As someone who gets frequent cold sores and has one copy of ApoE4, what should she do about it, if anything?
As the preceding discussion should illustrate, there is no “right” answer here. Like it is with so many therapeutic decisions in medicine, deciding a course of action is a matter of making probabilistic decisions with incomplete information, subject to change upon further data.
So, while I can’t dispense medical advice to newsletter readers, I will tell you what I would do if I were experiencing frequent cold sores (regardless of ApoE4 status):
Possibly Do → Anti-Viral Suppression Therapy
Daily anti-viral therapy is already considered safe and effective at preventing recurrent HSV2 (genital herpes) infections. The recommended dose for someone who isn’t immunocompromised is 1 gram per day.
So, were I experiencing recurrent cold sores, I would consider taking 1 gram per day of valacyclovir. I would then await the results of the clinical trials testing antiviral treatment for AD prevention, and modify my approach accordingly once the results were published.
Definitely Do → Pay Attention To Lifestyle
As we now know, HSV hides out in nerve cell bodies. It is thought that our immune system is what prevents it from spreading. Reactivation, when it does occur, happens when the immune system is weakened for one reason or another.
That weakening can be from diseases and medications that chronically suppress the immune system. HSV reactivation syndromes are more common in those who are chronically immunocompromised.
But our immune system is also weakened during times of stress. It owes its colloquial names (“cold” sore, “fever” blister) to the fact that outbreaks often occur in the midst of an infection by another micro-organism.
Additionally, inadequate sleep, overtraining, nutrient deficiencies, and acute psychosocial stress are all known to increase the risk of HSV recurrence.
In other words, many of the lifestyle factors that we know heighten the risk of AD also heighten the risk of HSV reactivation. So, tending to those factors is a win-win.
Thanks to Sarah for the excellent question (to submit your question for us, click here).
References
Cohen, Marc, Evan Austin, Stefan Bradu, and Jared Jagdeo. 2023. “The Association Between Herpes Simplex Virus and Alzheimer’s Disease: A Systematic Review.” Journal of Drugs in Dermatology: JDD 22 (10): 1046–52.
Devanand, D. P. 2018. “Viral Hypothesis and Antiviral Treatment in Alzheimer’s Disease.” Current Neurology and Neuroscience Reports 18 (9): 55.
Goldhardt, Oliver, Robert Freiberger, Tobias Dreyer, Luisa Willner, Igor Yakushev, Marion Ortner, Hans Förstl, et al. 2023. “Herpes Simplex Virus Alters Alzheimer’s Disease Biomarkers - A Hypothesis Paper.” Alzheimer’s & Dementia: The Journal of the Alzheimer's Association 19 (5): 2117–34.
Lövheim, Hugo, Jonathan Gilthorpe, Rolf Adolfsson, Lars-Göran Nilsson, and Fredrik Elgh. 2015. “Reactivated Herpes Simplex Infection Increases the Risk of Alzheimer’s Disease.” Alzheimer’s & Dementia: The Journal of the Alzheimer's Association 11 (6): 593–99.
Lövheim, Hugo, Jonathan Gilthorpe, Anders Johansson, Sture Eriksson, Göran Hallmans, and Fredrik Elgh. 2015. “Herpes Simplex Infection and the Risk of Alzheimer’s Disease: A Nested Case-Control Study.” Alzheimer’s & Dementia: The Journal of the Alzheimer's Association 11 (6): 587–92.